|
|
Gossypiboma
Submitted by Theresa Kaufman, MSIV
General Considerations
- Gossypiboma: retained surgical sponge
- From Latin “gossypium” (cotton) and Swahili “boma” (place of concealment)
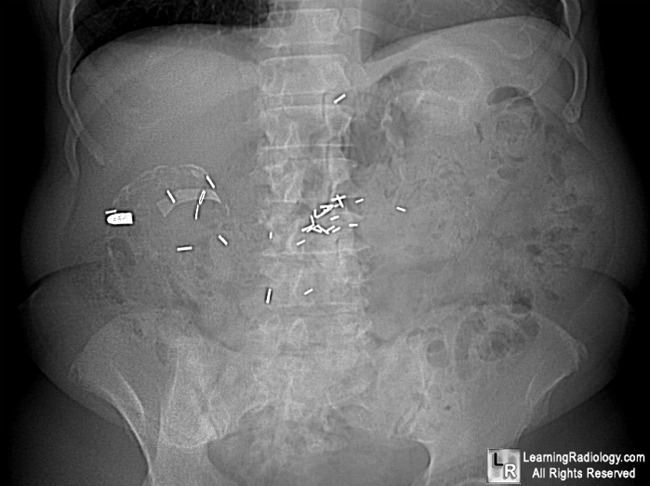
- Barium-saturated threads are woven into one side of all surgical sponges in the United States, allowing the sponges to be readily identified radiographically
- Usually appear as curvilinear densities, but may appear distorted if sponges have been folded
- Markers may deteriorate over time and may not be detectable
- Risk factors
- Long and difficult procedures, especially those with nursing/personnel changes
- Changes in operative field
- Emergency procedures
- Large body habitus
- Hemorrhagic procedures
- GI tract surgery and gynecologic surgery account for about75% of reported gossypibomas
- 40% are detected within 1 year of surgery
- 50% detected 5+ years after surgery
Clinical Findings
- May be very variable
- Exudative response early in the postoperative period
- Vague and nonspecific symptoms, or
- Symptoms of obstruction
- Changes in bowel or bladder function
Imaging Findings
- Conventional radiography
- Detection of radiopaque marker on sponge
- “Whirl-like” pattern of sponge
- Calcified mass
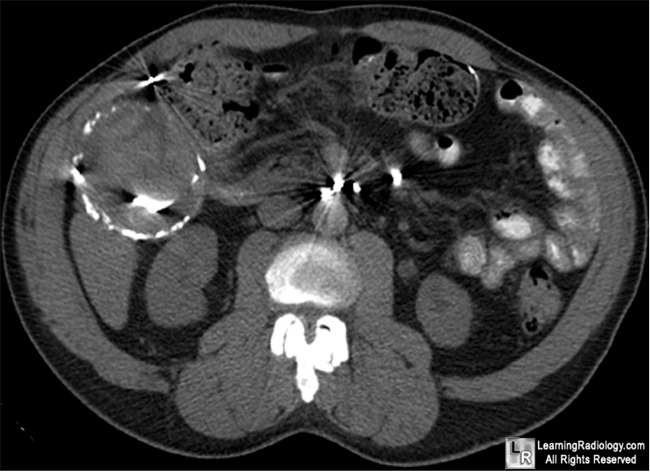
- CT
- Well-defined mass with soft-tissue attenuation
- Whorled appearance
- May contain gas bubbles within fiber meshwork
- Outer rim may contrast enhance
- May have peripheral calcification or calcification within mass
- US
- Echogenic “wavy” structure (sponge) within a mass with acoustic shadowing
- When acoustic shadowing is correlated with a palpable mass in the correct clinical setting, diagnostic for gossypiboma
- MRI
- Well-defined mass
- Capsule has low signal intensity on T1 and T2
- T1: variable signal density central fluid; low signal intensity nonenhancing sponge material
- T2: high signal intensity central fluid; whorled appearance of sponge material; low signal intensity peripheral rim
Differential Diagnosis
- Post-operative collection
- Abscess
- Hematoma
Treatment
- Complete exploration of site with removal of retained sponge
- Treatment of accompanying complications
- Drainage of fluid
- Treatment of fistulas or bowel obstruction
Complications
- Abscess formation
- Fistula
- Bowel obstruction
- Erosion into adjacent structures
Prognosis
- If diagnosed and removed in the immediate postoperative period, morbidity and mortality low
- Otherwise, major surgical interventions may be needed with increased risk of complications and mortality
- Overall mortality estimated at 11%-35% with a morbidity of about 50%


Gossipyboma. Retained surgical sponge. Red arrows point to marker on sponge.
The rim of the mass which formed around the retained foreign body has calcified (white arrows).
The patient was operated on years before for a gunshot wound.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here or here
Javors, Bruce R., and Ellen L. Wolf. Radiology of the Postoperative GI Tract. New York: Springer Verlag, 2003.
Haaga, John R. CT and MRI of the Whole Body. 5th ed. Mosby, 2008
|
|
|

{kind=link}
{kind=link}